Skimming papers
Nikhil Dhawan, MD
Created: 2022-04-05 Tue 13:54
1 Goals of lecture
- Understand the advantages of evidence-based medicine.
- How to skim a paper to see if it applies to your patients.
- Understand confounds and how studies remove them.
2 Why evidence-based medicine
- People vary considerably and the human body and it's diseases and their mechanisms are extremely complicated.
- Creating theories that can be predictive is a challenge especially in psychiatry.
- People are more complicated than a bridge.
- There are times in medicine we must rely on mechanisms and our primitive understanding of diseases and treatment.
- Observing if an intervention works in a particular population results in more reliable and certain treatments for our patients.
- In my opinion, finding, reading, and analyzing the empirical literature is necessary to practice ethically as a physician.
3 Positivism
- During medical school, you are taught a seemingly endless number of "facts."
- It may make one believe that what we need to do is learn all the facts of medicine.
- Unfortunately, medicine is constantly evolving.
- Today's treatments may be considered barbaric down the line.
- Although it's a challenge, try to change your way of thinking away from discrete facts.
4 A quote from Bradford Hill
The reactions of human beings to most diseases are, under any circumstances, extremely variable… ‘What the doctor saw’ with one, two, or three patients may be both acutely noted and accurately recorded; but what he saw is not necessarily related to what he did. The assumption that it is so related, with a handful of patients, perhaps mostly recovering, perhaps mostly dying, must, not infrequently, give credit where no credit is due, or condemn when condemnation is unjust. The field of medical observation, it is necessary to remember, is often narrow in the sense that no one doctor will treat many cases in a short space of time; it is wide in the sense that a great many doctors may each treat a few cases. (Hill, 1962; pp. 3–4)
5 A quote from Bradford Hill
Thus, with a somewhat ready assumption of cause and effect, and, equally, a neglect of the laws of chance, the literature becomes filled with conflicting cries and claims, assertions and counterassertions. It is thus, for want of an adequately controlled test, that various forms of treatment have, in the past, become unjustifiably, even sometimes harmfully, established in everyday medical practice. (Hill, 1962; pp. 3–4; my italic)
6 Looking at a paper (skimming guide)
- Similar to PICO methodology.
- You need to determine if the participants/patients studied in the trial generalize or are the same as the patient you are treating.
- You need to determine if it's the same intervention that you are trying (or similar to your intervention)
- You need to make sure it's the outcome you are looking for or a meaningful outcome.
7 Population/generalizability
- The first thing I do is look at the population and make sure that the results are generalizable to my population.
- For example, are these patients with schizophrenia in acute psychotic relapses?
- For example, are these patients with bipolar disorder in a manic episode? does it include bipolar 2 patients?
- I would argue hospitalized mania is different than outpatient mania.
8 Inclusion criteria of cariprazine study
- Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial
- Results: Use of cariprazine led to a greater least squares mean change in PANSS-FSNS from baseline to week 26 than did risperidone (−8·90 points for cariprazine vs −7·44 points for risperidone; least squares mean difference −1·46, 95% CI −2·39 to −0·53; p=0·0022; effect size 0·31).
9 Inclusion criteria of cariprazine study
- "a psychiatric history had to be available to ensure that patients had predominant negative symptoms and low levels of positive symptoms, and were therefore suitable for participation. Patients eligible for the study were adults aged 18–65 years who had a diagnosis of schizophrenia…, with onset occurring at least 2 years before screening. Patients had to be in a stable condition for at least 6 months before screening (ie, no psychiatric hospital admissions, acute exacerbations, or imprisonments) and meet the following clinical criteria: predominant negative symptoms for at least 6 months"
10 Inclusion criteria of cariprazine study
- "Patients whose condition was determined to be unstable and those with a PANSS factor score for positive symptoms (PANSS-FSPS) of more than 19 or a score increase of 25% or more during a lead-in period were ineligible."
11 Intervention
- Is the intervention the same as the one that I am giving or delivering?
- Look at how the medications are titrated? Did they get to a good dose? Is this similar to how I practice?
- Look at how often and the intensity of the psychotherapy given? Is this something that you can implement?
12 How DBT is delivered in the trial.
https://pubmed-ncbi-nlm-nih-gov.foyer.swmed.edu/16818865/
- "These functions are divided among the following 4 modes of service delivery: (1) weekly individual psychotherapy (1 h/wk), (2) group skills training (2½ h/wk), (3) telephone consultation (as needed within the therapist's limits to ensure generalization), and (4) weekly therapist consultation team meetings (to enhance therapist motivation and skills and to provide therapy for the therapists)"
- Therapists were asked to provide the type and dose of therapy that they believed was most suited to the patient, with a minimum of 1 scheduled individual session per week. Ancillary treatment could be prescribed as needed.
- Graph
{kind=link}
13 Aripiprazole and risperidone
- Aripiprazole, an antipsychotic with a novel mechanism of action, and risperidone vs placebo in patients with schizophrenia and schizoaffective disorder
- Results: Aripiprazole (20 and 30 mg/d) and risperidone (6 mg/d) were significantly better than placebo on all efficacy measures.
- Risperidone dosages were titrated upward (2 mg on day 1, 4 mg on day 2, and 6 mg/d for the remainder of the study) and administered orally after breakfast and after the evening meal. Aripiprazole was given as a fixed full dose orally after breakfast, with placebo given in the evening to maintain study blinding.
- https://pubmed-ncbi-nlm-nih-gov.foyer.swmed.edu/12860772/ (pdf here)
14 Outcome
- What are the outcome/results?
- Is it the outcome that's important to you?
- Is the difference between the arms a meaningful difference?
15 Intersept trial
- Methods: A multicenter, randomized, international, 2-year study comparing the risk for suicidal behavior in patients treated with clozapine vs olanzapine was conducted in 980 patients with schizophrenia or schizoaffective disorder, 26.8% of whom were refractory to previous treatment, who were considered at high risk for suicide because of previous suicide attempts or current suicidal ideation. To equalize clinical contact across treatments, all patients were seen weekly for 6 months and then biweekly for 18 months. … Suicidal behavior was assessed at each visit. Primary end points included suicide attempts (including those that led to death), hospitalizations to prevent suicide, and a rating of "much worsening of suicidality" from baseline.
16 Intersept trial
- Results: Suicidal behavior was significantly less in patients treated with clozapine vs olanzapine (hazard ratio, 0.76; 95% confidence interval, 0.58-0.97; P =.03). Fewer clozapine-treated patients attempted suicide (34 vs 55; P =.03), required hospitalizations (82 vs 107; P =.05) or rescue interventions (118 vs 155; P =.01) to prevent suicide, or required concomitant treatment with antidepressants (221 vs 258; P =.01) or anxiolytics or soporifics (301 vs 331; P =.03). Overall, few of these high-risk patients died of suicide during the study (5 clozapine vs 3 olanzapine-treated patients; P =.73).
17 Analyzing studies further
- If you restrict yourself to randomized controlled trials, then you are looking at fairly high-quality evidence.
- Be careful of meta-analyses and systematic reviews. They are only as good as the trials underneath them.
- Perhaps, the most important factor to look at when looking at a trial is confounding bias.
18 Confounding bias
- A third factor accounts for the association between two other factors.
- You see an effect between an intervention and the result, but actually there is a third factor that causes the effect.
- If you remove or account that third factor, the association goes away.
- This is more important than p values or "statistical significance."
19 Example of confounding bias
- Coffee drinkers are more likely than non-coffee drinkers to have cancer.
- Coffee drinking is associated with smoking. In other words, people who drink coffee are more likely to smoke, than non-coffee drinkers.
- Account for smoking, the association between coffee and cancer goes away.
- Although the association of coffee and cancer is statistically significant, it goes away when accounting for smoking.
20 Confounding bias
- Always think if there is another factor that may account or change the results.
- Be skeptical and doubt the paper as much as possible. Force the paper to convince you of it's results.
21 How to remove confounding bias
- You can remove confounding bias before the study with randomization.
- You can remove confounding bias after the study with a regression analysis (e.g., logistic or linear regression analysis)
22 Randomization example
- Give sertraline to half and placebo to half, but randomize who is in each group.
- Any particular difference between the groups, gets randomly equalized.
- Since people are randomly assigned there should be roughly the same number of women to men in each group.
- Same socioeconomic status, comorbidities should be equalized by using random assignment.
- You remove confounding bias even for confounds you may not know or think about or measure.
23 Table 1
- Table 1 of a paper shows the two arms of the study and their demographics.
- It tries to prove that the two arms are similar in their characteristics and that there are no confounds.
- It's possible that randomly there is a difference in the groups, and it's up to you to determine if the difference between the groups is meaningful.
- Sometimes p-values are used to show that there is no difference. This is a misuse of p-values. I look for about a ten percent difference.
24 Example
- You are looking if risperidone causes breast cancer.
- You randomize the sample to receive risperidone vs aripiprazole, but 70% of men are in the risperidone group and 70% of women are in the placebo group.
- You notice this in table 1 and realize that even with randomization this is a potential confound.
- You may conclude that risperidone prevents breast cancer given a decrease association.
- When you control for sex, the association reverses and risperidone is associated with breast cancer. (Simpson's paradox)
- https://pubmed-ncbi-nlm-nih-gov.foyer.swmed.edu/34474013/
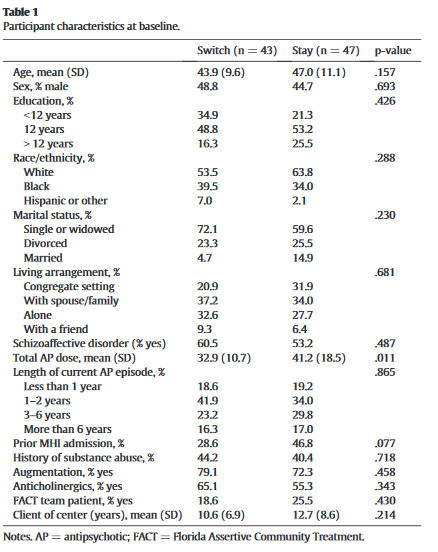
25 Example
- Discontinuing polypharmacy of antipsychotics.
- Results: Participants who switched to antipsychotic monotherapy experienced greater increases in symptoms than stay patients. These differences emerged in the second 6months of the trial. All-cause discontinuation rates over the 1-year trial were higher in the switch-to-monotherapy group than in the stay-on-polypharmacy group (42% vs. 13%; p<0.01). There were no differences in change over time in any of the side effect measures, except that stay patients experienced a greater decrease in Simpson Angus total scores than switch patients.
- https://pubmed-ncbi-nlm-nih-gov.foyer.swmed.edu/26141142/
26 Table 1
27 Another way to remove confounds - Regression analysis
- It's not feasible/ethical to force people at random to drink coffee for decades and the other group to drink placebo for decades.
- Therefore you can remove the smoking effect with regression analysis.
- Coffee drinkers and non coffee drinkers with cancer.
- Regression retrospectively removes confounds.
28 Regression analysis
- Essentially you put in possible confounds/factors into the computer and it controls for the confounds.
- The computer will let you know if the association goes away.
- The confounding factors that you are controlling for may be called covariates or use the term adjusted for.
- You can do this after you collect the data, but you need to collect data on the covariates as well.
- If they are using a "model" or "regression" analysis, then you can see what covariates or confounds they controlled for.
29 Example
- https://pubmed-ncbi-nlm-nih-gov.foyer.swmed.edu/34474013/ Adjusted for: substance misuse, previous suicide attempt, cardiovascular disease,
asthma or chronic obstructive pulmonary disease, diabetes; number of children; use of opioids, paracetamol, non-steroidal anti-inflammatory drugs, digoxin, spironolactone, statins, loop diuretics, beta blockers, calcium channel blockers, angiotensin system drugs, anti-parkinson drugs, tricyclic antidepressants, selective serotonin reuptake inhibitors, verapamil; duration of systemic hormone-replacement therapy use; and prolactin-sparing antipsychotic use.
30 How to approach journal club
- You have an excellent curriculum.
- Use journal club to teach you how to analyze studies.
- Don't expect to read landmark studies and learn the "truth" of psychiatry.
- The more experience you have on your own looking at studies, the more you'll get out of journal club curriculum.
- Have a goal of becoming comfortable enough to find and analyze studies to come to a conclusion you feel comfortable with to treat your patients.
- I'd recommend not making drastic changes to decision making based on one study. I look for multiple studies saying the same thing before making practice changes.
31 Read and search the literature
- Don't stop reading and searching PubMed! ! !
- Read the editorials or comments on the trial.
- They will analyze the paper and help you learn more about how to analyze papers.